With limited manpower and resources, hospitals can only do so much in a pandemic. Sadly, the country is still in the pandemic phase of the COVID-19 outbreak and more cases are expected to be confirmed in the following weeks. The Department of Health (DOH) has recently identified six areas in the Visayas as emerging COVID-19 hotspots. This includes Cebu City, Cebu province, Ormoc City, Southern Leyte, Leyte, and Samar. As of June 29, there are more than 7000 confirmed cases in Central Visayas, with Cebu City having the highest number of confirmed cases in the country.
Patients with COVID-19 sometimes develop severe and critical conditions that will warrant admission in the intensive care unit (ICU). The effective management of critically ill patients infected with COVID-19 is dependent upon the efficient provision of evidence-based nursing care. Notably, Eastern Visayas has only nine ICU beds while Central Visayas has 111. More than 50% of ICU beds in Central Visayas have already been occupied. Interestingly, the DOH, in consultation with the Philippine General Hospital, has recommended a 1:1 nurse-to-patient ratio for ICUs. Maintaining appropriate staffing in health care facilities, particularly ICUs, is essential to providing a safe work environment for health care workers and safe patient care. With the current state of local health systems in the Visayas, this “ideal” ratio will be hard to comply with, risking quality care and patient outcomes.
Early into the pandemic, the government was quick to anticipate this and published a call for nurse volunteers who are willing to provide their services to the designated COVID-19 referral hospitals. While this policy has the potential to increase the supply of health workers, particularly nurses, this might not be enough when we reach the peak of 75,000 COVID-19 positive cases expected to occur in the next few months.
The Cebu Medical Society has raised its concerns over the city’s exhausted and overwhelmed health system citing health workforce shortage and scarcity of medical equipment. More than 130 health care workers in Central Visayas have been infected with COVID-19 as of June 15. Some hospitals have forced their nurses to undergo home quarantine after being exposed to positive cases. Consequently, this left the hospitals with a skeleton staff that is just enough to keep essential services running.
The surge of confirmed cases leading to an increase in demand for nursing services has significantly strained local health care systems. This expected surge of confirmed COVID-19 cases will now require the restructuring of policies to address the nursing workforce shortage in hospitals, particularly in intensive care units. Therefore, it is imperative for the government to seek ways on how to increase the capacity of the health care system, primarily by improving nursing resource management in hospitals. A combination of national- and hospital-level policies could be the key to solving this workforce problem.
Despite the efforts of the Department of Health to increase health workforce supply through volunteerism, there is a great potential that the program will not be able to adequately address the growing demand for nursing services, specifically intensive care nursing. Therefore, there is an urgent need to look at other policy alternatives that can complement this program alongside other policies.
POLICY ALTERNATIVES
The increase in service demand should be coupled with an increase in service supply. The government must ensure that hospitals are adequately staffed with competent nursing personnel that can deliver quality care to the people. Policies to make the necessary arrangements to ensure adequate staffing needed to respond to the increased demand for nursing services should now be taken into consideration. The recommendations provided below could hopefully give the government and nursing administrators a new perspective on how to address the imminent workforce shortage.
Status Quo: Emergency Hiring and Redistribution of Existing Staff
Current policies for managing the current issue on localized nursing workforce shortage are limited to the redistribution of existing staff from various sources and the temporary employment of volunteer nurses. Earlier this year, the DOH announced that it is hiring health personnel in select hospitals and other health facilities to expand the country’s response to the COVID-19 pandemic.
As of July 1, DOH Central Visayas has deployed 270 nurses across different facilities in Cebu City. Meanwhile, the Armed Forces of the Philippines has deployed nine nurses as a response to the shortage. In addition to this, nurses under the Nurse Deployment Program were also redeployed to DOH- and LGU-operated hospitals. Some NDP nurses, however, were retained in their original areas of assignment to help implement public health measures to prevent and control the spread of infectious diseases.
Alternative 1: Issuance of Temporary Licenses to Graduate Nurses
Through the Professional Regulation Commission and the Board of Nursing, with the recommendation of the Secretary of Health, the government can issue temporary professional licenses to nursing graduates and be classified as Graduate Nurses (GN). Similar to policies in the United States of America, the issuance of temporary licenses will permit Graduate Nurses to render nursing services to patients in non-COVID units. This will allow professional nurses to be deployed to critical care units flooded with confirmed cases of COVID-19.
Temporary licenses will only be given to individuals who have been conferred the degree of Bachelor of Science in Nursing by a reputable institution of higher learning in the Philippines. Individuals applying for temporary licenses may or may not have taken the nurse licensure examination; provided, that no applicant must have taken the licensure examination for more than three times. Successful applicants will be assigned to hospitals that have requested additional staffing complement due to shortages.
Alternative 2: A Tiered Staffing Policy for Pandemics
The government can direct public and private hospitals to adopt a tiered staffing strategy. This staffing strategy, adapted from the Society of Critical Care Medicine and the Ontario Health Plan for an Influenza Pandemic, can help address the need to staff inpatient and ICU beds by making use of existing nurse clinicians. This can be supplemented by other clinicians assuming new roles, students who were given temporary licenses, and resigned or retired personnel returning to work.
In this model (Figure 1), a registered nurse who is trained or experienced in critical care and who regularly manages ICU patients oversees the care of two to three groups of three to four patients each. A non-ICU nurse who has some ICU training or experience but does not regularly perform ICU care is inserted at the top of each triangle. This non-ICU nurse extends the knowledge of the ICU nurse while working alongside other members of the team without ICU training and experience. The tiered staffing policy can be an effective strategy to incorporate non-ICU-trained staff to augment the trained and experienced ICU staff.
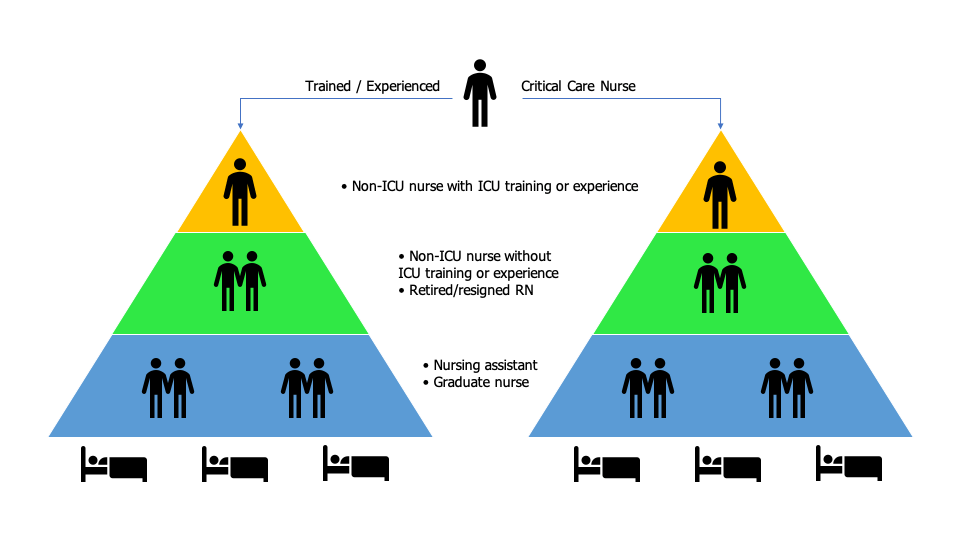
Figure 1. Tiered staffing model for critical care units
Less-skilled staff will have to assume roles previously performed by critical care nurses under the direct supervision and support of the latter. Nursing tasks may need to be delegated to less specialized workers such as nursing aides and ward assistants. Allowing this approach will reduce the responsibilities of the critical care nurses but it does not remove the accountability from these nurses. Critical care nurses remain responsible for any task delegated to lower-level cadres or non-critical care staff under their supervision.
POLICY ANALYSIS AND MATRIX
Status Quo: Emergency Hiring and Redistribution of Existing Staff
Public and private institutions have recruited retired, resigned, and unemployed nurses to help in the management of probable or confirmed cases of COVID-19 admitted in hospitals. This was supplemented by the redeployment of nurses from the military and those under the Nurse Deployment Program of DOH. These strategies effectively increased the number of available nurses for hospitals in the Visayas.
These strategies were economically efficient in that the government did not incur additional costs except for the health worker benefits prescribed by the Department of Health and the Bayanihan to Heal as One Act. Moreover, these strategies were easy to administratively implement as they fall within the mandate of local government units and the DOH. Further, these strategies enjoy political and social acceptance as they can address problems with coverage and access to health services, particularly nursing services.
These strategies, however, may not be enough to maintain the adequate supply of competent nurses with experience and training in critical care. Not all nurses will have the skills and knowledge needed to care for patients in ICUs. These strategies fall short in this aspect of the workforce shortage. Currently, no data is available on how many of the recruited and redeployed nurses have training and experience in critical care nursing.
Alternative 1: Issuance of Temporary Licenses to Graduate Nurses
DOH Department Order No. 2020-0169, which allows medical graduates to engage in the limited practice of medicine as deputized physicians, sets a precedent for this policy alternative. Moreover, R.A. No. 11469 vests in the President the power to engage temporary Human Resources for Health to complement or supplement the current health workforce. However, the issuance of nursing licenses and certificates of registrations falls under the jurisdiction of the Board of Nursing as stipulated in Republic Act No. 9173 or the Philippine Nursing Act of 2002. Only the Board has the authority to issue, suspend or revoke certificates of registration for the practice of nursing in the Philippines. As such, this alternative will require a stringent policy process that will take time before a sound policy can be considered. Nonetheless, this should not hinder the government from considering this policy option when the worst scenario is bound to happen.
This alternative can be effective in increasing the number of available nurses that can render health services. Reallocation of program budgets will be required to finance the compensation of Graduate Nurses as well as in instituting licensing procedures. A salary amounting to Php22,316/month, which is equivalent to Salary Grade 11, can be considered adequate compensation for a Graduate Nurse. Should the government decide to hire at least 100 nurses to maintain a 1:1 ICU nurse-to-patient ratio in Eastern and Central Visayas, the government will need to allocate 2.2 million pesos/month for salaries alone. The table below shows the direct costs associated with hiring a Graduate Nurse in varying durations of engagement with government hospitals.

While this can be an efficient and effective strategy, hiring Graduate Nurses to assume the roles of Registered Nurses in hospitals is not very popular among patients and their caregivers, especially when complex procedures are involved. Past experiences, however, show that Filipinos are more accepting of student nurses and graduate nurses practicing basic nursing skills such as bed bath, wound care, and health teaching.
Alternative 2: A Tiered Staffing Policy for Pandemics
As opposed to other strategies, a tiered staffing policy will not result in an absolute increase in the number of nurses in hospitals. While the level of care may not be the same as in the typical ICU in non-crisis times, having care directed by trained and experienced critical care nurses is an effective way to maximize care for large numbers of critically ill patients. This approach with critical care nurses supported by additional staff members would increase a hospital’s capacity for care of critically ill patients. The use of this approach can help achieve or maintain a safe nurse-to-patient ratio in both general wards and critical care units.
With this alternative, no additional costs will be incurred by the government. Rather, it will only require the reorganizing of hospitals’ staffing management, particularly for nurses. It is technically and administratively feasible as this policy veers closely with the team-based approach which nurses are very familiar with.
This alternative may not need to go through the usual policy process engaged in creating national policies. The policy can emanate from the Centers for Health Development or local government units. Patients and their caregivers do not see this policy option as a hindrance to quality care. Rather, the policy sets a mechanism to improve access and coverage in critical care services while ensuring patient safety and quality of nursing services. Currently, no law or statute prohibits the institution of this kind of policy. It can serve as a quick fix to the local nursing shortage.
POLICY RECOMMENDATIONS
Cebu remains a high-risk area, which means that the SARS-CoV-2 is still spreading in the province. A study conducted by some professors of the University of the Philippines projects 15,000 cases in the province by the end of July. However, relaxing quarantine measures may cause an escalation of up to 30,000 cases by July 31. The occupancy of beds in Cebu City alone, where the majority of hospitals in the region are situated, is more than 70% while occupancy of ICUs is more than 60%. More than 4% of nurses in the Central Visayas region still cannot render services because they were either admitted to the hospital or quarantined in their homes or other health facilities.
Given this, the following stepwise recommendations based on this policy analysis should be considered to augment the required staffing patterns in intensive care units / critical care areas in Central and Eastern Visayas. The government should continue the emergency hiring of health workers which will result in an absolute increase in the number of available nurses. Because not all nurses have adequate training or experience in critical care nursing, this should be supported by a policy on tiered staffing. Such a policy will maximize the skills of critical care nurses while ensuring the delivery of quality nursing care to more patients. Lastly, should human resources for health become severely depleted due to sickness, death, and other reasons, the government should explore the option of issuing temporary licenses to graduate nurses.
- Issue a policy on tiered staffing
The government should enact local policy that will designate nurses with training and experience in critical care nursing as interim unit heads overseeing the care of two to three groups of critically ill patients. Each group of less specialized staff (i.e. nurses with inadequate ICU training and experience, nursing assistants, graduate nurses) will assume roles previously performed by critical care nurses. Moreover, hospitals should allow task shifting to less specialized health workers such as nursing aides and ward assistants to reduce the workload of registered nurses.
Additional training for less specialized workers in areas of potential increased service demand should be provided to ensure staff competency and capacity, especially when deployed to critical care areas. Procedures for supervision and monitoring of performance should be established to ensure the quality of services delivered.
- Continue hiring nurses from various groups
Retired, resigned, and unemployed nurses should be continuously recruited to help in the management of probable and confirmed cases of COVID-19 that are admitted in hospitals. Training and orientation should be provided to meet the needed minimum skill sets. Moreover, procedures for credentialing newly recruited staff, specifically looking at training and experience in critical care nursing, must be developed.
The government can also tap nursing organizations such as the Association of Private Duty Nurse Practitioners of the Philippines whose self-employed members are hired to care for private individuals and/or their families. More nurses from the military and police services can be deployed to civilian hospitals. NDP nurses should remain in their original area of assignment to help in the implementation of public health measures.
- Issue temporary licenses to graduate nurses
The Board of Nursing can issue temporary licenses to Graduate Nurses within a prescribed period (e.g. 90 days or until the pandemic is controlled) that will allow them to care for patients in non-COVID units. This will allow the reallocation of trained and experienced nurses to critical care units. Graduate Nurses can work under a tiered staffing approach where they are supervised by competent registered nurses.
Procedures for credentialing, training, and performance evaluation should be developed in consultation with members of the academe and nursing service administrators. The Board should also develop procedures for revocation of temporary licenses that can be done at a time the government deems the pandemic is under control or until hospitals are at the level of or below their surge capacities.
CONCLUSION
The role of nurses has been considered crucial in managing this pandemic, most especially in implementing strategies to #flattenthecurve. While this is the case, shortage in the nursing workforce will not make the management of the pandemic any easier. Hence, the government and hospital administrators need to plan ahead of time to address pending problems such as nursing shortage and to increase the capacity of the health system to cater to the growing needs of the population.
Effective nursing workforce management is essential to ensure adequate staff capacity and competency during a pandemic which substantially increases the demand for nursing services. The recommended stepwise approach can be a promising solution to the local nursing workforce shortage. However, these recommendations are interim solutions to a possibly chronic nursing workforce shortage in the Philippines. A national investment in the nursing profession will be vital to address this shortage. Such investment will require significant political will, support, and financial investment.
REFERENCES:
1. Aguilar, K. (2020). Gov’t allows ‘limited practice’ of medical graduates in COVID-19 response. Retrieved 5 July 2020, from https://newsinfo.inquirer.net/1258334/govt-allows-limited-practice-of-medical-graduates-in-covid-19-response
2. COVID-19 FORECASTS IN THE PHILIPPINES: NCR, CEBU and COVID-19 HOTSPOTS as of June 25, 2020. (2020). Retrieved 5 July 2020, from https://www.up.edu.ph/covid-19-forecasts-in-the-philippines-ncr-cebu-and-covid-19-hotspots-as-of-june-25-2020/
3. DOH RELEASES INTERIM GUIDELINES FOR EMERGENCY HIRING OF HEALTH PERSONNEL Press Release/12 April 2020 | Department of Health website. (2020). Retrieved 5 July 2020, from https://www.doh.gov.ph/doh-press-release/DOH-RELEASES-INTERIM-GUIDELINES-FOR-EMERGENCY-HIRING-OF-HEALTH-PERSONNEL
4. DOH TO DEPUTIZE MED GRADS TO ASSIST IN NAT’L COVID-19 RESPONSE | Department of Health website. (2020). Retrieved 5 July 2020, from https://www.doh.gov.ph/press-release/DOH-to-deputize-med-grads-to-assist-in-nat%E2%80%99l-covid-19-response
5. Duque: 22 more doctors to be deployed to Cebu City. (2020). Retrieved 5 July 2020, from https://www.sunstar.com.ph/article/1862123/Cebu/Local-News/Duque-22-more-doctors-to-be-deployed-to-Cebu-City
6. Einav, S., Hick, J. L., Hanfling, D., Erstad, B. L., Toner, E. S., Branson, R. D., … & Christian, M. D. (2014). Surge capacity logistics: care of the critically ill and injured during pandemics and disasters: CHEST consensus statement. Chest, 146(4), e17S-e43S.
7. Emerging Health Workforce Strategies To Address COVID-19 | Health Affairs. (2020). Retrieved 5 July 2020, from https://www.healthaffairs.org/do/10.1377/hblog20200414.197056/full/
8. Goh, K. J., Wong, J., Tien, J. C. C., Ng, S. Y., Duu Wen, S., Phua, G. C., & Leong, C. K. L. (2020). Preparing your intensive care unit for the COVID-19 pandemic: practical considerations and strategies. Critical Care, 24, 1-12.
9. Halpern, N. A., Tan, K. S., & SCCM, V. T. (2020). US ICU resource availability for COVID-19. Society of Critical Care Medicine, March, 25.
10. IN NUMBERS: What hospitals need to treat COVID-19 patients. (2020). Retrieved 5 July 2020, from https://www.rappler.com/newsbreak/in-depth/256133-numbers-what-hospitals-need-treat-coronavirus-patients
11. Nonato, V. (2020). Not Enough Beds, Healthcare Workers To Address COVID-19 Cases In Case Of Surge – UP Research | OneNews.PH. Retrieved 5 July 2020, from https://www.onenews.ph/not-enough-beds-healthcare-workers-to-address-covid-19-cases-in-case-of-surge-up-research
12. Phua, J., Weng, L., Ling, L., Egi, M., Lim, C. M., Divatia, J. V., … & Nishimura, M. (2020). Intensive care management of coronavirus disease 2019 (COVID-19): challenges and recommendations. The Lancet Respiratory Medicine.
13. Shang, Y., Pan, C., Yang, X., Zhong, M., Shang, X., Wu, Z., … & Sang, L. (2020). Management of critically ill patients with COVID-19 in ICU: statement from front-line intensive care experts in Wuhan, China. Annals of Intensive Care, 10(1), 1-24.
NOTE: This is an abridged version of an academic paper submitted to the faculty of the Department of Health Policy and Administration, UP College of Public Health.
